

The BMI Deep Dive
Common sense on the controversial health metric.
Post summary
BMI—a measurement that estimates body fat based on your height and weight—has recently been criticized in popular articles in outlets like the New York Times and Prevention.
And many influencers and athletes say BMI is “worthless” because athletic people can have a BMI that classifies them as “overweight.”
But the truth is much more complicated.
BMI is valuable—if we understand its purpose and the surprising facts around BMI. Understanding BMI can help us make smarter health decisions.
Warning: This post is long, deep, and research packed. But hopefully it will give you a more measured, nuanced appreciation of how body size influences your risk of disease, fitness, and more.
Housekeeping
This post, like all Monday posts, is free to all subscribers of Two Percent.
But only Members get full access to Wednesday and Friday Two Percent posts and their audio versions. Become a Member below:
ICYMI:
On Wednesday, we ran a post exploring the truth about ultrarunning tribes. The reason can improve your endurance and mindset.
On Friday, we revealed the four best trail shoes (which also work great for hiking and rucking) in Gear Not Stuff.
Audio/podcast version
The Post
The New York Times recently published a piece titled “Time to Say Goodbye to the B.M.I.?” It criticized Body Mass Index, a calculation that estimates body fat based on your weight and height.
Stories like this come around once a year. A couple years ago it was a story from Prevention, whose headline stated, “Why we’re saying goodbye to BMI.” The story explained that the magazine would no longer use Body Mass Index (BMI).
You’ve probably also encountered critics of BMI online. For example, an Olympic rugby player recently went viral for suggesting BMI is useless.
BMI is a public health metric we use to assess disease risk. Using our height and weight, BMI classifies people as “normal weight,” “overweight,” or “obese.” It’s recently come under fire from some media outlets, online health gurus, and athletes who argue that BMI is a poor measure of health for a few reasons.
One criticism is that people can have an “overweight” or “obese” BMI and still be healthy and athletic.
Another is that BMI doesn’t consider where a person’s extra weight is coming from or stored.
This means that, for example, a weightlifter might be “overweight” because he or she has relatively more muscle. Some outlets have even argued that BMI is racist.
The anti-BMI movement seems to be resonating. For example, I referenced BMI in a newsletter a few months ago. Afterward, a reader emailed me to say that my use of BMI diminished the legitimacy of the information because BMI has been “debunked.”
But rather than disregard BMI, it helps to understand it. If we can better understand BMI, we can make more informed decisions about our health.
Warning: Today’s post is long. But BMI is a critical topic worth understanding. If you’re pressed for time, listen to the podcast on 1.5x speed.
We’ll cover:
What BMI is
Where BMI came from
Why we use BMI
What people get wrong about BMI
Whether there is an “optimal” BMI
Whether BMI is racist
If other health metrics might be better
Why there’s so much pop media controversy around BMI
How you should use this information
A final take on BMI
On Wednesday, we’ll explain whether it’s OK to have an “overweight” BMI if your extra weight is from muscle. I.e., We’ll look at how much muscle is healthy.
What is BMI?
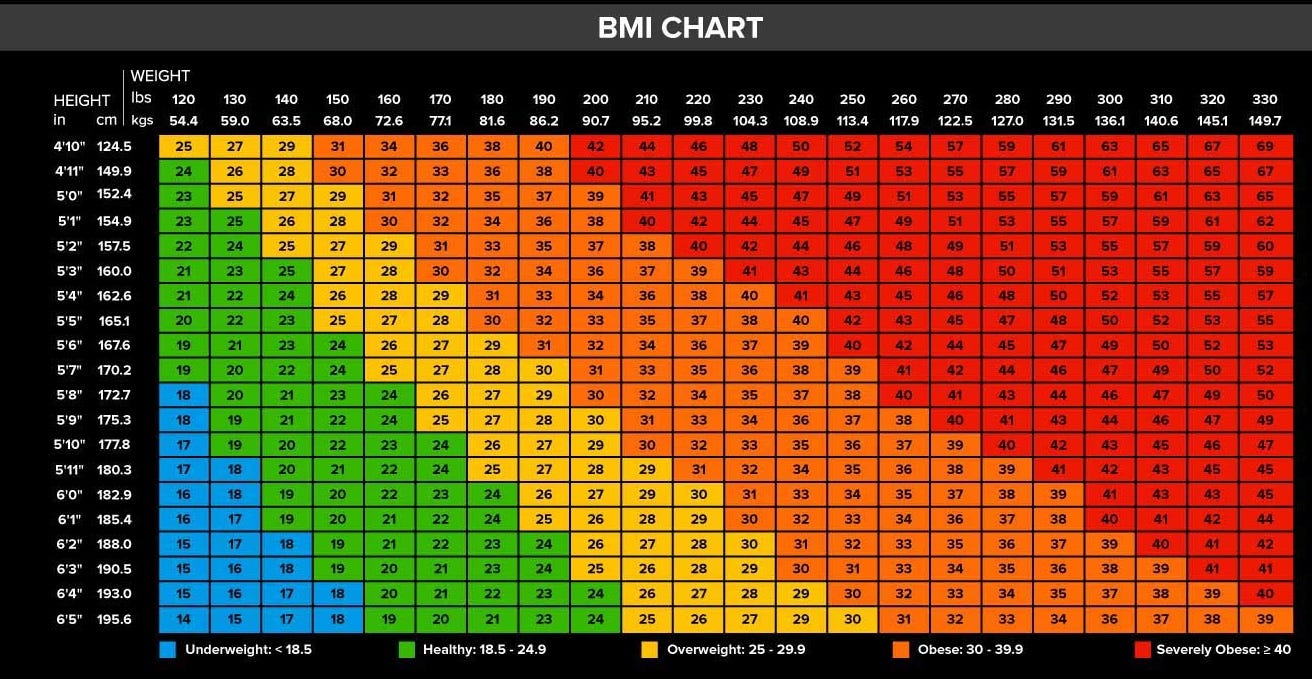
It’s a simple calculation that assesses your weight status based on your height. Calculate yours here.
A BMI under 18.5 puts you in the underweight category.
If your BMI is from 18.6 to 24.9, you’re considered “normal” weight.
If you score from 25 to 29.9, you’re considered “overweight.”
Above 30 and you’re considered “obese.”
Anything above 40 is considered “extremely obese.”
Where did BMI come from?
In the 1900s, the insurance industry noticed more death claims from their heaviest policyholders. So a statistician at the Met Life Insurance Company found a solution.
He developed a simple table using height and weight the company could use to quickly figure out the risk level of its policyholders.
It worked rather well. So well that doctors began using it to guide their patients.
By the 1970s, the medical and research community fully adopted the idea. They called it the Body Mass Index, or BMI. It's been used by the world’s most influential health organizations and research institutions ever since.
Why do we use BMI?
It’s a simple, quick, and free tool for public health researchers and doctors to assess a population’s risk for weight-related diseases.
Imagine if a doctor wanted to get a perfect sense of her patient’s health status. What would she do?
To assess the patient’s heart disease risk, she might take an echocardiogram.
To assess cancer risk, she might take various imaging screenings, like a CT scan.
To assess sleep quality, she might do a sleep apnea test.
To assess bone health, she might do an arthritis screening. And on and on.
But doctors don’t do that. Performing all those tests would be time-consuming and expensive (extremely expensive).
Instead, at your annual checkup, she takes simpler tests. She takes your height and weight. She asks you if you smoke and if anything is bothering you. She checks your blood pressure, does some basic blood work, and maybe a couple of other things.
Your doctor uses your height and weight information to calculate your BMI. From there, she can quickly gauge your risk of many health problems. For example, here are some numbers:
Up to 20 percent of cancer is attributable to having a BMI over 30. A New England Journal of Medicine study concluded, “the absence of excess body fatness lowers the risk of most cancers.”
A BMI of 30 or above increases your risk of Type II diabetes by more than 200 percent.
Having a BMI over 25 makes you anywhere from 15 to 103 percent more likely to develop heart disease. (It’s the number one killer of Americans). One study found that for each one-point increase in BMI, heart failure risk rises 5 percent for men and 7 percent for women.
People with a BMI greater than 30 are 680 percent more likely to develop knee arthritis compared to people who score in the “normal” BMI range. The data suggests that 69 percent of knee replacements and 27 percent of hip replacements are attributable to having a BMI of over 25. This is likely why one study found a drop in BMI of 2 or more units decreased the odds of developing knee osteoarthritis by more than 50 percent.
Having a BMI between 25 and 30 increases your risk of death anywhere from 7 to 20 percent. BMIs between 30 and 40 are associated with anywhere from a 45 to 90 percent increase in death. A BMI over 40, which is considered “extremely obese,” is associated with a 300 percent greater risk of death. This data is from a 14-year study. It followed 4 million adults who were disease-free at the beginning of the research period.
Problems due to a high BMI are growing globally. More than two billion people are now obese by BMI standards. And “between 1990 and 2017, the global deaths and (years of living in disease) attributable to high BMI have more than doubled for both females and males,” found one study.
BMI is obviously less in-depth than tests like an echocardiogram or CT scan.
But it’s free and simple and can tell you about your risk for many different health problems. The above list is just a sampling.
BMI is also critical in emergency medicine. Emergency rooms use it to quickly determine how to effectively ventilate, medicate, and feed patients in critical care. This saves lives.
Another upside: Unlike blood work or some complicated scan, anyone can use BMI to determine their risk level. For free. In 10 seconds. No doctors or medical machines or needles involved—and, most beautifully, the person won’t have to haggle with the insurance company afterward.
That person can even determine their own treatment, too. BMI higher than you’d like? Lose weight. Too low? Gain it.
This makes it an especially useful tool for public health departments in developing countries where medical access and treatment is poor.
What do people get wrong about BMI?
The New York Times article criticized BMI for only being able to show correlations. That is correct. But that’s precisely what BMI is designed to do.
BMI is a population health measurement. It cannot accurately tell us any one person’s exact odds of any given disease (factors like genetics, exercise, leanness, and so much more alter that risk).
Instead, BMI measures how body weight impacts the disease risk for most people most of the time. But these broad strokes allow us to make rational estimations about health risks.
For example, let’s say you had a group of 100 normal-weight women and a group of 100 obese women.
The research shows that the risk of heart disease for a normal-weight woman is 22 percent, while it’s 39 percent for an obese woman.
This means that 22 of the 100 normal weight group would likely get heart disease while 39 of the 100 obese women would.
The important points here:
Being in a “normal” BMI doesn’t mean you’re risk-free. You still have a one in five chance of heart disease.
Meanwhile, being obese doesn’t automatically mean you’ll get disease. You can still be healthy. It just means your risk is greater.
To put it another way: Disease is something of a gamble—and having a high BMI seems to load the dice in favor of disease.
Considering how many diseases are related to BMI … that’s a lot of rolls with loaded dice. This is why people with higher BMIs tend to live shorter lives.
Dr. Walter Willett, the legendary epidemiologist, put it this way: “Controlling weight, after not smoking, is the single most important factor for a long, healthy life.”1
The fact that BMI is only a correlation shouldn’t be controversial. The same type of population data is behind every other health recommendation.
For example, the lifetime risk of lung cancer for nonsmokers is about 1.5 percent. For smokers, it’s about 13 percent.
Just because you don’t smoke doesn’t mean you’ll avoid lung cancer. But smoking is also not a guarantee that you’ll get lung cancer.
Yet do we think this makes anti-smoking campaigns useless? Of course not. Smoking raises your risk.
One other criticism of BMI is that the cutoffs are arbitrary. Critics ask why scientists chose 25 and above to be considered “overweight” instead of, say, 26 or 27.
But the word “arbitrary” seems to imply that scientists arrived at the number by, like, tossing a dart at a dart board.
The cutoffs are based on decades of research. Scientists look at the research and make rational decisions based on it. (We’re also now starting to modify BMI cutoffs based on race. More on that below.)
Dr. Christopher J.L. Murray, Ph.D., is arguably the world’s brightest mind around health metrics. He ran the WHO’s Evidence and Information for Policy Cluster and Harvard’s Initiative for Global Health and Center for Population Development Studies. He put it like this:
Body mass index is one of the best studied health risks that we have in the Global Burden of Disease – through hundreds of cohort studies, some of them really quite large, like the CPRD study in the UK that alone had about 30 million person-years of observation.
When you put all these studies together, there are 60 million plus person-years of observation that tell us about the relationship between body mass index and the risk of some 30-plus diseases, cardiovascular diseases, diabetes, a long list of cancers, and some musculoskeletal disorders. And the relationship between BMI and a number of those disease outcomes is not only well studied but extremely strong.
Most diseases are also based on cutoffs. For example, heart disease, diabetes, some cancers, and more.
Take diabetes. A person whose blood sugar after an overnight fast is 99 mg/dl or lower isn’t diabetic. But if a person’s level is 100 to 125, they’re prediabetic. If they register 126, or higher then they’re diabetic.
Those cutoffs are just like BMI. And like BMI, some people who have a blood sugar level that makes them diabetic may not suffer disease symptoms while others might.
Is there an optimal BMI?
Someone submitted this question to me via Instagram, and my answer was, “optimal for what?”
For health and longevity, Murray (the WHO, Harvard, and University of Washington researcher) said: “We know that the risk is lowest for a BMI somewhere between about 22 and 25.” But if your goal is sports performance, a higher BMI might be better.
For example, one study found the top marathoners have an average BMI of 19.8. But top throwers usually have a BMI between 30 and 34 (technically obese).
If you want to find the ideal BMI for your own sport, look at how its best athletes are built and make some estimations.
We’ll go in depth on how much muscle is good for health on Wednesday.
Is BMI Racist?
Outlets like Scientific American, Good Housekeeping, and The Huffington Post have recently run stories exploring whether BMI is racist.
The idea is that BMI cutoffs are based on socially constructed beauty standards and that because the initial data used to construct BMI came from white men, many historically marginalized groups have been hurt. The implications and takeaways from the articles are that certain groups of people (if not everyone) should ignore BMI.
Different races may indeed have different disease risks at different BMIs. For example, a few studies have found that Asian populations have more complications from obesity at a lower BMI.
This means that a person of Asian descent with an obese BMI would be at more risk of disease compared to someone of another race who has the same BMI. Which is why the World Health Organization recently adjusted the obesity cutoff points for people of Asian descent.
Some doctors also suggest that Black women could be marginalized or inappropriately diagnosed because they tend to have slightly higher BMIs compared to white and Hispanic women yet carry less body fat for a given BMI. One study even found that Black women could be healthier at a higher BMI.
This is why Fatima Cody Stanford, an obesity researcher at Harvard, has proposed further adjustments to BMI.
Her group looked at a massive governmental databank that included racial background and disease. Her conclusion: The BMI cutoffs for Black, White, and Latino men should be lower (meaning, for example, that a man would be considered “obese” at a BMI of 29 or above instead of 30 or above).
For White and Latino women, cutoffs would also shift downward. But for Black women, the cutoff would be increased (for example, to 31 and above for obesity instead of 30).
With this in mind, there are two schools of thought on whether we should keep or ditch BMI because of questions around race.
The first argues that telling people to ignore BMI is a bad idea. In response to the Scientific American article, The Harvard scientists Maraton-Flier, Rexford S. Ahima, and Jeffrey S. Flier wrote:
Rather than focusing on black patients being inappropriately diagnosed (by BMI) with obesity as a consequence of racism, we are most concerned that black individuals with obesity may go untreated because they do not receive quality health care or are denied effective therapies.
Like many health indices, the BMI is imperfect. But it is neither racist nor useless. If doctors become reluctant to use this important tool out of misplaced concern over its supposed racist origins, they would only succeed in harming the health of the most vulnerable minority populations—including many African-Americans.
If we were to stop using BMI for more personalized metrics, they believe, it may even force more expenses of time and money on populations who are already vulnerable. Doctors might instead use an expensive test that leads to bigger hospital bills.
The Harvard researchers explain, “in the years since it was first introduced, the BMI has been assessed—and validated—as an indicator of serious health risks in a great variety of gender, racial and ethnic groups.” This is why the World Health Organization uses the metric.
The second school of thought sees BMI as hurtful, especially to historically marginalized groups. It views BMI as part of a system of oppression that exacerbates health disparities. This occurs because BMI labels people as “overweight” or “obese.”
From there, negative societal implications around fatness make it even harder for disadvantaged groups to get better and more nuanced care.
As this debate continues, racial differences are being studied extensively. They’ve shown that some races do tend to have different risks at different BMIs.
They’ve also shown that having a higher BMI puts most people at greater risk of health problems regardless of their background. We still need to learn what BMI matters most under what conditions and why. Science is a process, not a destination.
In the meantime, the nation’s most prominent researchers of obesity and race, like Fatima Cody Stanford and Jamy Ard, think BMI is here to stay until we find something better.
Ard, a researcher at Wake Forest, told the Washington Post: “We’d love to have a better marker that actually gets at the physiologic state of the fat cell. Until that point, this (BMI) is what we have as a way to at least initiate conversations and start to talk about some general treatment strategies.”
Why does BMI get so much criticism in the media?
Good question. BMI is relatively uncontroversial among leading health organizations. The American Heart Organization, CDC, Ivy League Medical schools, the World Health Organization, and other institutions worldwide use it when appropriate.
I worked at a leading health magazine for many years and had a few ideas about why major outlets might run such a strongly anti-BMI piece.
It gives media outlets something new and counterintuitive to say about health, which is a slow-moving field.
Counterintuitive and controversial stories generate more clicks and, therefore, money for media outlets.
Journalists often lack a scientific background and, due to the modern economics of media, are required to publish more stories in less time.
I texted a friend who is an executive-level editor at one of the world’s largest health magazines. She said this:
I might argue that an era ago, media had to limit their emotional responses to deal in facts as much as possible. Then the social media era led humans to act and speak on emotion all too easily. And media took on an important role to arbor all that emotion with facts.
But media wanted more, so it’s essentially now trying to make emotional stands and follow the social media crowd instead of leading it or acting as arbiter of it. Many (anti-BMI articles) are emblematic of that trend and that problem.
The media wants to grab at an audience’s emotions. They want to BE the news instead of reporting the news. This drives more clicks. To be the news you must be willing to ‘take a stand.’
In other words, for articles to play well on social media—which is inherently emotion, hot take, and outraged-based—you need to create articles that favor emotion, hot takes, and outrage over nuance and balance.
Is a high BMI OK so long as I exercise?
A Cochrane Review (basically the gold standard for reviewing medical science) concluded: Exercise is associated with improved cardiovascular disease risk factors even if no weight is lost.
If you’re overweight or obese, exercising will decrease your risk of certain diseases. (Note: It’s also possible that exercising while overweight or obese might increase your risk of some problems like joint pain. Exercise selection becomes important … this is why I’m such a proponent of rucking).
Then again, if you are in the obese category of BMI, losing weight and exercising will decrease your risk of all diseases even more.
But getting too deep into these risk factors misses something about life and living it.
Remember that having an “overweight” or “obese” BMI doesn’t guarantee early death and disease. And maybe you find that the lifestyle changes it would take you to drop your BMI into the normal category just aren’t worth it.
The diet and exercise might detract from your life so much that your days are a bit less bright. In that case, it’s a rational decision to not drop your BMI.
Yes, your risk will be relatively higher. But you can accept that and also accept that decreasing your risk may not be worth it to you. Remember: an overweight or obese BMI isn’t a death sentence.
What should I do if my BMI says I’m overweight or obese?
If you’re concerned about it, I’ll tell you what a doctor and expert told me: Go see your doctor and ask them for appropriate tests that are deeper than BMI.
Are there any other simple tests that are more accurate than BMI?
Maybe. Some scientists also think the waist-to-hip ratio is promising. A few studies have found that it’s a better predictor of disease risk than BMI, while others have suggested that it’s worse.
The New York Times article identified the Body Roundness Index as another option.
The idea is that, when done correctly, those tests better accounts for build and muscle mass. A person who was lean with more muscle yet had a high BMI, for example, would have a lower hip-to-waist ratio.
This is important because where your fat is stored influences your health. Fat stored around your belly and waist is likely to indicate more fat around your organs and, therefore, an elevated risk of disease.
To measure hip-to-waist ratio:
Wrap a tape around your middle, halfway between the bottom of your ribs and the top of your hips.
Breathe out, relax and pull so it’s taut but comfortable.
A measurement over 40 inches is a sign to speak to your doc and get a full assessment.
Not all doctors love this test, though. It takes more skill. And your waist circumference can fluctuate massively depending on water retention, resting muscle tone, breathing mechanics, what you ate, the last time you went to the bathroom, and more. Those could all lead to inaccurate data.
Murray said this about those tests:
People have proposed other measures like the waist-to-hip ratio, direct measurements of adiposity. And there are small studies – instead of millions of person-years of observation, we’re talking about 50,000 or less person-years of observation – that suggest that some of these other measures, like waist-to-hip, may be even better predictors of some outcomes than BMI.
We don’t yet have the data at the population level to come close to assessing whether that’s really true at a broad level when you only have a few thousand or tens of thousands of person-years compared to millions for BMI. It’ll take a lot more evidence to show that that’s statistically more powerful than BMI as a predictor of outcome.
Best case: Keep both your BMI and hip-to-waist ratio where you want them to be and you’ll have less to worry about.
Final Take
Is BMI perfect? No, and it wasn’t meant to be.
But that doesn’t mean it isn’t useful and informative. We should continue to research its application to different groups while understanding that half a century of good data shows high BMIs put most people at greater risk of disease.
Until we find something equally good that’s simple and free and that anyone can use, medical experts think it’s worth keeping around—and using as just one measurement among many to make public health recommendations.
Have fun, don’t die, BMI,
-Michael
Sponsored by Momentous
Momentous made me feel good about supplements again. Over 150 professional and collegiate sports teams and the US Military trust their products, thanks to the company’s rigorous science and testing. I don’t have the time or desire to cook perfectly balanced meals that give me all the necessary nutrients and protein I need (let’s face it, few of us do!). So I use their Recovery protein during hard workouts; essential multivitamin to cover my bases; creatine because it’s associated with all sorts of great things; and Fuel on my longest endurance workouts on 100+ degree days here in the desert (because Rule 2: Don’t die). And I also love (love!) that Momentous is researching and developing women-specific performance supplements.
**Use discount code EASTER for 15% off.**
Sponsored by Inside Tracker
Your blood holds stories—lots of them. It can reveal critical information about your risk of heart disease, your metabolic health, recovery, endurance, inflammation, and much more. And yet, to get the most important information, you need to go deeper than the lab work your doctor has you do each year.
Enter Inside Tracker, created by researchers at Harvard, Tufts, and MIT. They make it easy to get deep blood work, providing analysis that can tell you about risks in your future and help you make guided decisions that will help you live and perform better, longer. Results from my own tests led me to alter a few health habits, and I’m better for it.
**Use discount code EASTER.**
Sponsored by GORUCK
When I decided to accept sponsorships for this newsletter, GORUCK was a natural fit. Not only is the company's story included in The Comfort Crisis, but I've been using GORUCK's gear since the brand was founded. Seriously. They've been around ~12 years and I still regularly use a pack of theirs that is 11 years old. Their gear is made in the USA by former Special Forces soldiers. They make my favorite rucking setup: A Rucker 4.0 and Ruck Plate.
**Use discount code EASTER for 10% off**
Here I’d add that exercise is also important for health. The message: Don’t be too big, don’t smoke, move often.
Beautiful post that I’d love to see trending online but it made me feel good rather than outraged so I expect it to just kick ass on substack and not pop up in recommended reads online.
I think one reason why there’s so much push-back on BMI is that “overweight” and “obese” are socially loaded words. Especially for the health conscious, these terms denote failure. So, this is where nuance from potentially confounding factors like exercise become important.